
You are already tired of reading about this damn coronavirus. I’m also tired of writing about it. The last time was six months ago (about the Delta variant). The match is getting tough. At times we have been playing on the grass, with the virus close by. Also cheering for our team from the stands, watching the virus from a distance. Referee! The time is over! We are cold, our ass is frozen, we are hungry, we need to pee. We were late for an appointment. The cost of the parking is going to be expensive. Your child is bored. You are bored too. The game is not over. Your head is full of small worries. Concerns that would disappear if this coronavirus match is won at once. But SARS-CoV-2 team set Omicron on the pitch. It could have been called Fu, or Fa, but its name is Omicron. Omicron plays as an attacking player and has the 11 on his back. Scary. In the Greek alphabet, Xi is right before Omicron. Xi is not scary. But the president of China is called Xi and, having in mind those who speak of the «Chinese virus», the WHO skipped Xi and took to Omicron.
Omicron enters the pitch like a bull. You rub your ass to warm it up, zip up your jacket, and sit down again. In silence, as you warm your child and rub his back, asking yourself: Omicron? Where the hell did it come from?
After almost two years of the pandemic, there is such amount of information that anyone, from deniers and conspiracists to catastrophists, can find the data, verified or not, that fits their extreme reasoning. This blog intends to use an experience in reading biomedical articles to digest information and send it from the band as a soft cross so that you can finish it with your own head.
Where did Omicron come from?
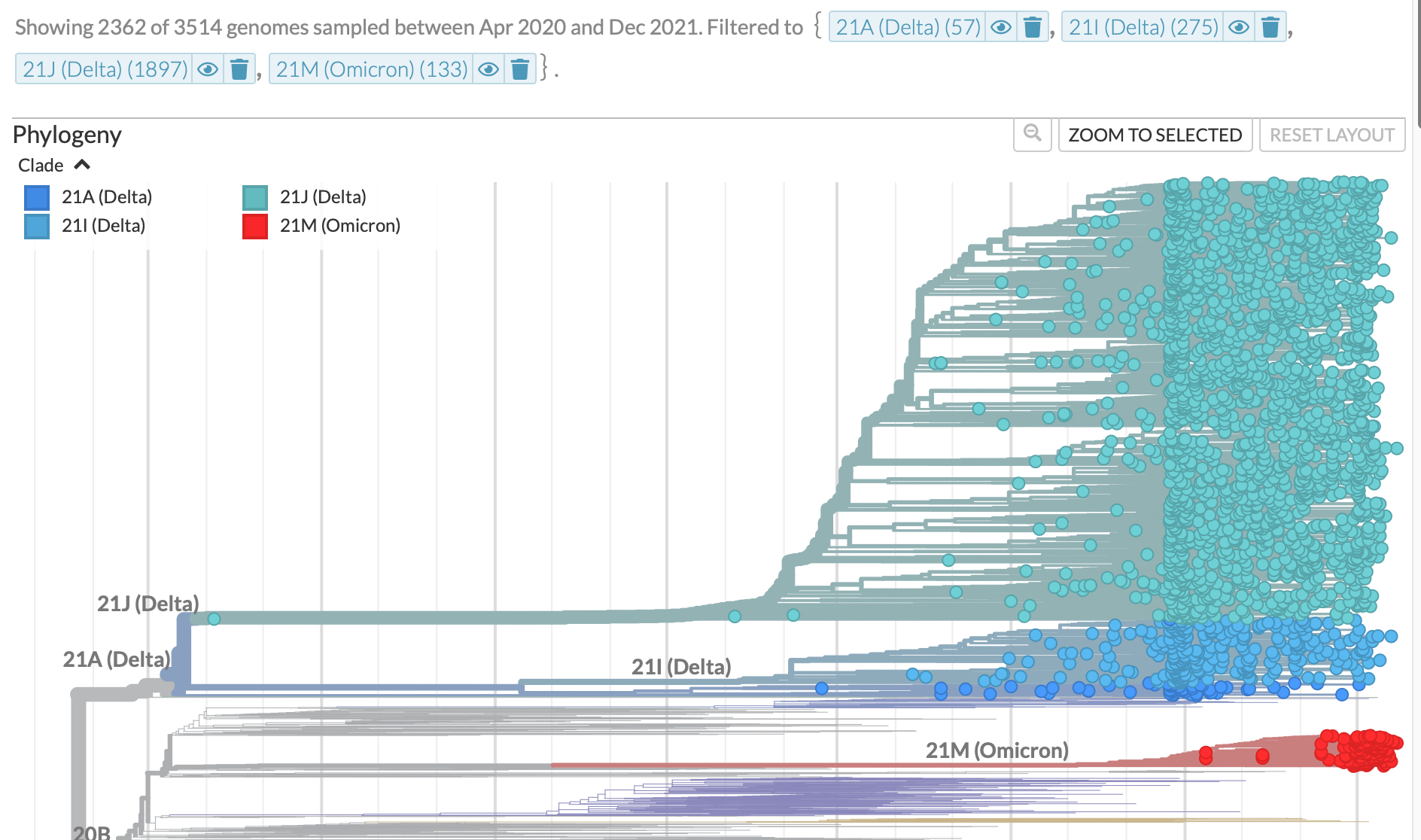
Omicron appeared out of nowhere. The GISAID database accumulates more than six million sequences of the SARS-COV-2 virus sent by scientists from different parts of the world. This information allows building a phylogenetic tree of the virus where each branch represents a change in its sequence. In this way, we saw how the Delta variant accumulated mutations, consolidating some and adding others, witnessing the progressive birth of its thirteen mutations. Omicron suddenly came out onto the pitch with about fifty mutations. Where did Omicron come from? —scientists also wonder.
One of the hypotheses is that Omicron arose from the recombination of viruses from different lineages. However, data from Viana and colleagues do not support such possibility. Another hypothesis is that Omicron evolved on a single immunosuppressed individual. For example, on an AIDS patient without his/her medications to reinforce the immune system. Within a patient with chronic COVID-19, the virus can evolve for months to create a variant that later passes to another individual through contagion. In such a case, GISAID scientists would not detect the intermediate variants. It is not a proven hypothesis, but it is a plausible hypothesis because genetic changes of the virus (up to 30) have been observed in people with permanent infection for months. And because there are about 8 million people with AIDS in South Africa, and about a third of them do not have access to medication that restores their immune system.
Another hypothesis is that Omicron comes from a country where the virus is not tracked. Only 89 countries submit SARS-CoV-2 sequences to the GISAID database. Thus, for example, the virus could not be traced if it was cooked in Tanzania and reached South Africa later. This highlights the importance of universal access to science and technology for global health. And, of course, the importance of vaccinating everywhere to minimize virus spreading and evolution since this is a global threat.
We did not see Omicron coming, just like Jamie Vardy was not seen coming. At 23 he was playing for an amateur team, working in the steel industry to survive, until he was signed by F.C. Halifax Town to play in the English 7th division. At the age of 25, after playing for 5th division Fleetwood Town F.C. and scoring 31 goals in 36 games, he was signed by 2nd division Leicester. At the age of 28, he was elected the best player in the Premier League and played the Euro with England. At 29, 2017-2018 season, he won the Premier League with Leicester scoring 20 goals.
Omicron was also nobody until November 19 when samples from COVID-19 patients were sequenced in South Africa. These sequences were uploaded to GISAID on November 23. On November 24, South Africa notified the WHO that it had detected a very special variant with 50 mutations compared to the original virus. 30 of these mutations were in the spike proteins, which are the keys to entering human cells. Given such a rate of mutations, the WHO took two days to classify it as a variant of concern. By November 30, Omicron was already in eleven countries at least. As of today (12-24-2021), Omicron is the predominant variant in many areas, and models predict that it may displace the Delta variant across the globe by January. Omicron is Vardy. Omicron came out of nowhere to be a world star.


And how does Omicron play? Is dangerous?
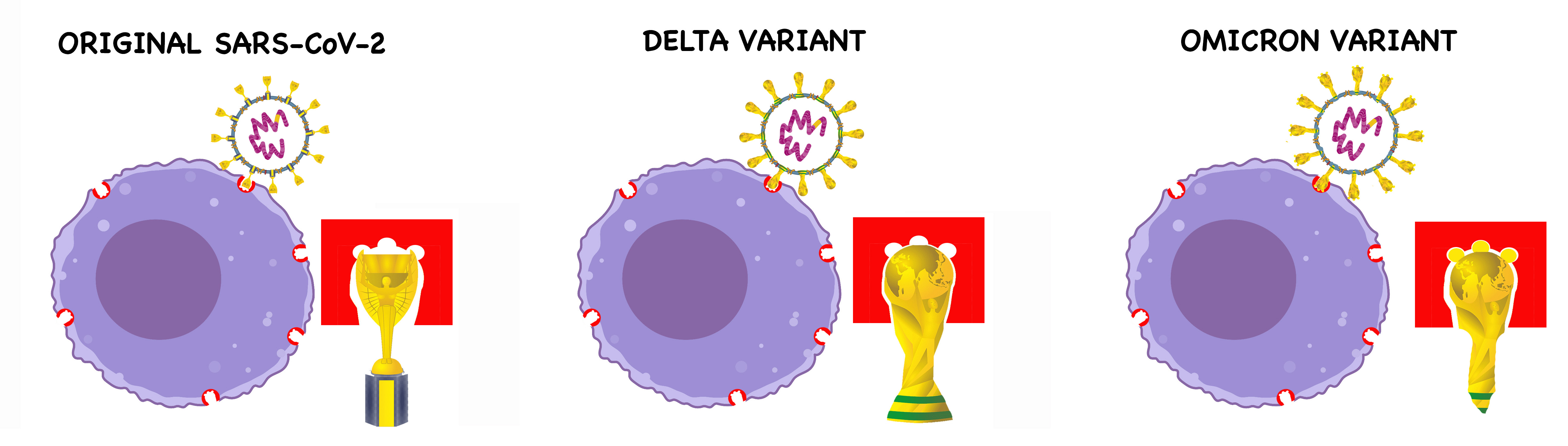
Last summer, using the World Cup, I explained the changes in the spike protein of the Delta variant that favoured its anchoring to receptors mediating virus entry into some human cells. At that time, we wondered if the Delta variant could be improved. Omicron has come up with 30 mutations in the spike protein to give us an answer. So changed is the virus that Omicron escapes the recognition from some of the antibodies we have. But could it be that so many changes also offer some advantage to humans?

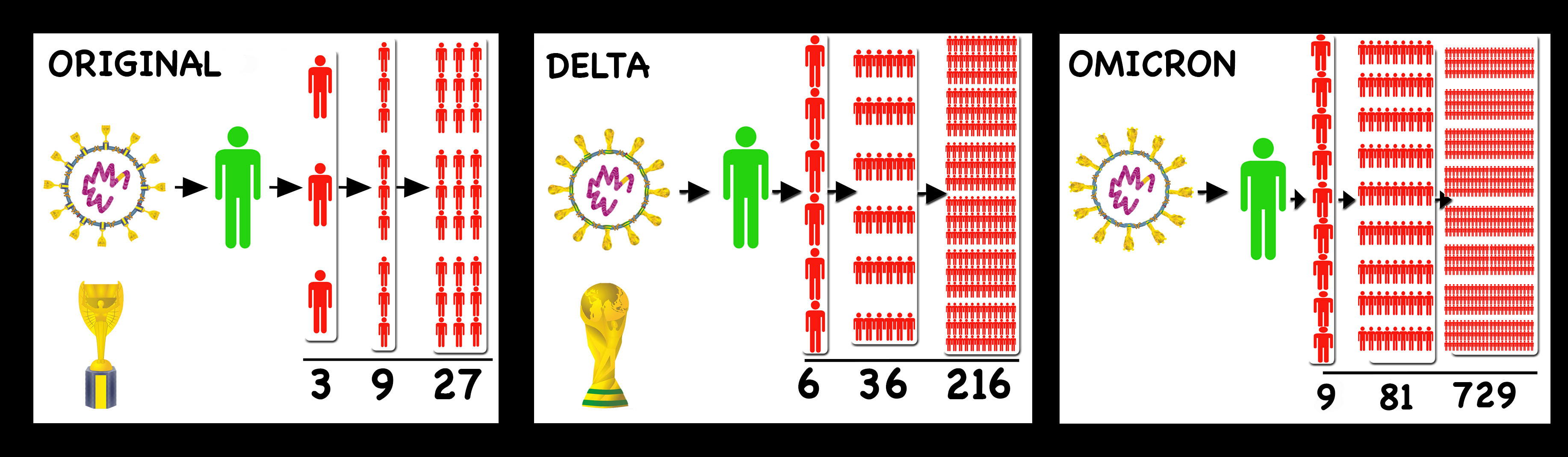
The SARS-CoV-2 coach has made the Omicron for Delta substitution at a time that hurts Humanity Athletic. Just before Christmas! Omicron is fast spreading, with a higher basic reproduction number Ro, causing a wild exponential increase if we do not take measures. According to Martin Hibberd, professor of infectious diseases at the London School of Hygiene & Tropical Medicine, if the original SAR-CoV-2 had a Ro of 2.5 and a Delta of 6, Omicron could go as high as 9 or 10 (if we do not take measures against the virus). To understand what the increase in Ro meant in the spread of the virus, in a previous article of «COVID-19 told through football» we explained it with people giving away tickets. If we consider that Omicron has a Ro of 9, in just three cycles of contagions we would have more than 700 infected. In five cycles, people with COVID-19 will not fit in Anfield Stadium.

The identification of the Omicron variant coincided with an exponential increase of cases in the Gauteng province of South Africa. The rate of positives among Gauteng’s tested inhabitants went from less than 1% in early November to 35% by the end of November. That was not a good sign. Omicron spread rapidly through the rest of the country and into neighbouring Botswana. Infections doubled every 1.8 days. Weekly cases were five times more with Omicron than with Delta, which was still circulating. What had worked to control Delta, did not work to control Omicron. Omicrón infections also affected people vaccinated or with previous COVID-19 although with less severity than in unvaccinated. Therefore, its greater contagion capacity could be due not only to better transmissibility but also to an escape of the neutralizing antibodies produced by the vaccines or by having passed the disease.
Some scientists did not sleep much lately to do experiments that give us some light in the darkroom in which we find ourselves locked with Omicron. For example, the serum of vaccinated people can be used to measure the activity of their antibodies to neutralize Omicron, and to know the ability of our T lymphocytes to kill cells infected with Omicron. Let’s start with the good news: T lymphocytes deal well with the variant change in vaccinated people, recognizing 70% of their targets after infection with Omicron. So we maintain the basal defence with our killer cells or T lymphocytes. The bad news is that several research groups have found that the antibodies of vaccinated people, or who had the disease, are less effective and only a percentage of those antibodies maintain their neutralizing capacity against Omicron. However, we can partially repair this issue with booster doses.
Is Omicron more dangerous than Delta?
The virus can mutate and improve for its convenience, but there are two points to take into account: (i) its capacity for improvement is finite and limited by its own nature. (ii) The virus, from an evolutionary point of view, is interested in spreading itself, not screwing up your life. The virus doesn’t give a damn about us. Therefore, the virus may be interested in a variant with a better transmission but less pathogenic. So there is a possibility that this pandemic virus becomes something that becomes part of our lives like a headache, a cold, or Bayern Munich winning the Bundesliga.
Science needs time. What is known about Omicron is preliminary, as it could not be otherwise in a variant over a month old, but a study from the University of Hong Kong indicates that Omicron replicates much faster in cells of the bronchi and more slowly in lung cells. This could have a positive implication on the severity of the disease. In this direction, a group from the University of Cambridge has shown that lung organoids (models) are less infected with Omicron than with Delta.
The information about Omicron surpasses us and we find conflicting news. We have to wait to be certain about the severity of Omicron infections, but for now, we can look at places that are a little ahead of the wave of Omicron infections. The million-dollar questions are:
Is Omicron More Dangerous Than Delta?
Do vaccines protect us against Omicron?
Here you can find four studies by teams from the United Kingdom, South Africa, and Denmark that indicate that Omicron infections are less likely to end with hospitalization.

South Africa. Wolter et al. (12-22-2021)
Those infected with Omicron are 80% less likely to be hospitalized but beware, once hospitalized they have the same risk of suffering from severe COVID-19. In South Africa, there are fewer vaccinated (40% of the population) but a high percentage of the population has immunity from previous infections.


United Kingdom.
Fergunson et al. (12-22-2021) (England)
40-45% reduction in the risk of hospitalization (one day or more) after infection with the Omicron variant compared to the Delta. The study was conducted between December 1 and 14, with 56,000 cases of Omicron and 269,000 cases of Delta.
Sheikh and Collaborators (12-21-21) (Scotland)
Patients infected with Omicron have a two-thirds reduction in the probability of being admitted compared to those infected with Delta.

Denmark. Holm Hansen et al. (12-22-2021)
Vaccine efficacy drops 30% with the Omicron variant. Vaccines are less effective as time passes after vaccination, but efficacy improves with a booster dose.
In summary:
Even being vaccinated, we are more susceptible to being infected with Omicron than with Delta, and the probability of contagion increases as time passes from the second dose. What served to protect us from Delta may not work for Omicron.
A booster dose partially restores protection against Omicron.
If you are vaccinated or have had a previous infection, a contagion with Omicron seems to be less likely to end in hospitalization.
Everything is so recent that we would have to wait a few weeks to see if the increase in infections caused by Omicron translates into an increase in hospitalizations and deaths. For now, the data are encouraging, but the cases of infections are so high that, even if a smaller percentage of people go to hospitals, we could saturate health systems.
How do we defend ourselves against Omicron?
Booster dose
In addition to the shields that we already know (masks, ventilation, test, caution), we have booster doses of vaccines to recharge the deposit of neutralizing antibodies, even though Omicron escapes a percentage of these antibodies.
There are books to explain mathematics through soccer, and to analyze soccer through mathematics. The maths required to understand the need for a booster dose is to calculate percentages. If the percentage of antibodies that works against Omicron is lower, a booster dose that increases the number of antibodies will make that percentage higher.
If only 20% of the antibodies against old SARS-Cov-2 variants neutralize the Omicron variant, having 100 antibodies only 20 would be useful. As an example, a booster dose of Moderna (half dose compared to the original dose) can increase your amount of antibodies 40 times. Then, after your third dose you would have 4000 total antibodies, and 800 useful instead of 20. So a booster dose is recommended to combat Omicron, for those vaccinated and for those not vaccinated but previously infected.
- Booster doses of Pfizer or Astrazeneca also increase the number of antibodies.

Test
The tests are still very important because they allow stopping the transmission by isolating the individual testing positive. Now we have antigen tests for sale everywhere that tell us in 15 minutes if we are contagious or not. Remember that antigen tests are less sensitive than PCR, but accurate when you have a high viral load and are more contagious. Antigen tests are a snapshot of the moment, so it is advisable to do them just before an event to protect attendees from a possible case of supercontagion. Should everyone be tested just before an indoor dinner party? Well, at least those who notice any symptoms compatible with COVID-19, or who have doubts about whether they could be infected somewhere a few days before.
Other things to keep in mind regarding antigen testing:
- Most tests detect the virus N protein (nucleocapsid), which is not as mutated in the variants as the spike protein. So most antigen tests DO WORK for Omicron.
- In vaccinated people, the first symptoms are the consequence of a response to the vaccines. Therefore the high viral load can arrive 2 or 3 days after these symptoms. The correlation symptoms = high viral load is no longer as clear as at the beginning.
- Since Omicron replicates faster, you can test positive earlier (3-4 days after infection) than after infection with previous variants.
- They give false negatives, but they give positive when it matters most (when you’re contagious)
Follow @michaelmina_lab for more info about antigen test
Vaccination of children
In recent months there are more cases of infections in children. It may be that the mutations that the virus accumulates facilitate infection in minors. As a father, my points in favour of vaccinating my 7-year-old daughter are: (i) I provide her with extra help to defend herself against the virus in case of contagion, (ii) I help reduce community transmission of the virus, and (iii), I reduce the weight of concerns if she is infected since the virus can continue to mutate, and previous vaccines would always protect, partly at least, from the newest virus variant. Yes, by vaccinating my daughter I expose her to an amount of spike protein, but it is a controlled dose, approved by clinical tests, and applied to millions of children already.
Making decisions about a child is not easy at all for parents. I imagine the weight of responsibility on Messi’s parents, accepting their eleven-year-old son’s treatment with a growth hormone that had been tested in a clinical trial with fewer than 200 children. Messi’s parents accepted that he was treated for years, and even they pricked him with this hormone. It is estimated that Messi grew between 10 and 15 centimetres thanks to the treatment. Trusting science did not go wrong at all in this case.

Antiviral pills
On the other hand, Pfizer has created a drug, recently approved by the FDA. According to the clinical trial, Paxlovid reduces hospitalization or death by 88% if administered within the first five days of infection. The question is whether the production and distribution capacity will be enough to supply the entire planet. Pfizer says it could produce 30 million boxes of pills by mid-2022, and the United States has already bought 10 million. Remdesivir, another antiviral, is also approved by FDA. The company Merck has another antiviral called Molnupiravir that could be approved by the FDA in the next few days, although the results of the clinical trial for COVID-19 are not as spectacular as those of Paxlovid. These new antiviral pills could be a fantastic winter signing, like the one Liverpool made at Christmas 2011 by signing Luis Suárez from Ajax for 26 million euros. Suárez scored 82 goals in 113 games for Liverpool.


Omicron may have greatly improved his abilities to transmit, but at the cost of losing other qualities. Perfection has not been seen in football, and it is difficult to see it in a virus. But if the virus is not weaker, our team has tools to combat it and has no limits to improve as SARS-CoV-2 has. For example, Moderna and Astrazeneca have already announced that they are working on specific vaccines against Omicron. These vaccines could be produced in a short period of time because only the RNA (Moderna) and DNA (Astrazeneca) sequences would have to be changed. In several places (as ex. US, Spain), scientists are working on a intranasal vaccine that would provide sterilizing immunity. Finally, to continue fueling optimism, although in places like the United Kingdom; United States, or Spain the curve of Omicron infections grows steeply, South Africa has already managed to double it. Yes, it is possible!

The match is not over
The main concerns from the beginning of this pandemic were to protect our elders and not saturate health systems. The first objective appears to be accomplished and stable with booster doses. To know if we can solve the second one, we need to wait a few weeks. Omicron could take a smaller percentage of people to the hospital but infect too many people. We already knew Delta. Now we need time to know Omicron. Does Omicron use both legs? Does Omicron shoot from outside the box? Which side does Omicron take to dribble on? We know almost nothing. It seems that the symptoms of Omicron are somewhat different, that it does not affect taste and smell, that its first symptoms, lessened by the effects of vaccines, are mistaken for the common cold. Time. We need time. Meanwhile, we keep walking on the wire, maintaining the balance between economy, social life and health. Studies confirm that stress, anxiety, depression and suicide have increased. You have to be careful, but you have to live. From our bench, governments and institutions direct us with protocols that are sometimes contradictory. You go from the pitch to the stand, and from the stand to the pitch. On the pitch, now watching Omicron pass by your side and slowing down his game. In the stand, taking a breath and waiting for the minutes of this game to pass. You are tired. Bored. Your child is bored too. Your ass is frozen and you need to go to the bathroom. You want to leave the stadium. But we are better than the virus, and we are a team. And then you hold on. Calm! Calm! -you say to yourself. You go to pee, buy something to eat, and go back to your place in the stand. You put newspaper on the cold seat and sit while you feed your child a snack and hug him. «It will end soon»-you tell him. You don’t know it, but you tell him. And then you go down to the grass, where the virus is. And there you are, great player, standing up to Omicron because you are better than him and because your team needs you. Because, although it may not seem like it, we are dominating this game and we know that our victory is a matter of time. Because we are going to defeat this virus and we are going to celebrate it.
@CeronLab
@raticosdefutbol
