
When Wuhan gave the initial whistle back in January 2020, the game against the SARS-CoV-2 coronavirus seemed a dull match in the Humanity F.C. schedule. However, SARS-CoV-2 locked us down at home during the first part. Once we learned how the rival can hurt us, the game was balanced in the second half, and we reached extra time. Then, after a year of match, Humanity F.C. reacted by dropping the vaccines onto the pitch. It was thought that vaccines would not arrive on time, but they did. In the last six months, SARS-CoV-2 has received many goals and is not comfortable in the game. Although everything indicates that the virus will lose the match, the matches must be secured as soon as possible to avoid complications and surprises. In fact, the extension is lengthening because there are Humanity F.C. players who do not pass the ball to the decisive vaccines. On the opposite side, the SARS-CoV-2 has brought out the Delta variant. Delta is a fast and elusive attacker who is nagging and worrying. Where the fuck did this Delta variant come from? We did not see it at the SARS-CoV-2 bench.

Where do the variants come from?
Variants arise because the virus mutates. By making replicas of its genetic material (RNA), the virus makes mistakes that are mutations. A minority of these errors cause some of the viral proteins to change their shape or properties slightly. Sometimes, hese changes can give the virus an advantage. When the virus gets a good mutation, the virus keeps it. With SARS-CoV-2 viruses worldwide and replicating massively, the likelihood of several good mutations coming together in the same virus increases over time. The possibility of a top player coming out of a soccer school is very low. But if you have an extensive network of scouts and the most prominent soccer academy in the world, the chances of having several good players on the same team increase. Thus, the Chinese investment group Evergrande built an elite academy for some 2,500 children (about 200 girls), chosen from all over China. They practice football six days a week in its facilities with 42 football fields. At the school entrance, a replica of the World Cup reminds them of the final objective. Over time, they’ll have increased chances of accumulating 3 or 4 top players, not more than 10 or 14 years apart, in the same team. Thus, in football/soccer, as in the viral world, large numbers and perseverance make the improbable probable, such as China winning one of the next soccer World Cups.
If we stop contagion worldwide, we reduce the chances that the virus will improve to make a fantastic team with great mutations.


The Delta variant is already the most abundant on the planet.
And the Delta variant of the SARS-CoV-2 virus appeared, which maintains some good mutations for the older variants and adds other mutations that improve its skills to propagate. In just four months, Delta has become the dominant variant globally (79% of all SARS-CoV-2 viruses are Delta, according to https://nextstrain.org/ncov/gisaid/global, at the beginning of August). It is so «good» that it will retire other variants of the game. See the evolution of the Delta variant (turquoise blue) in this animated map:
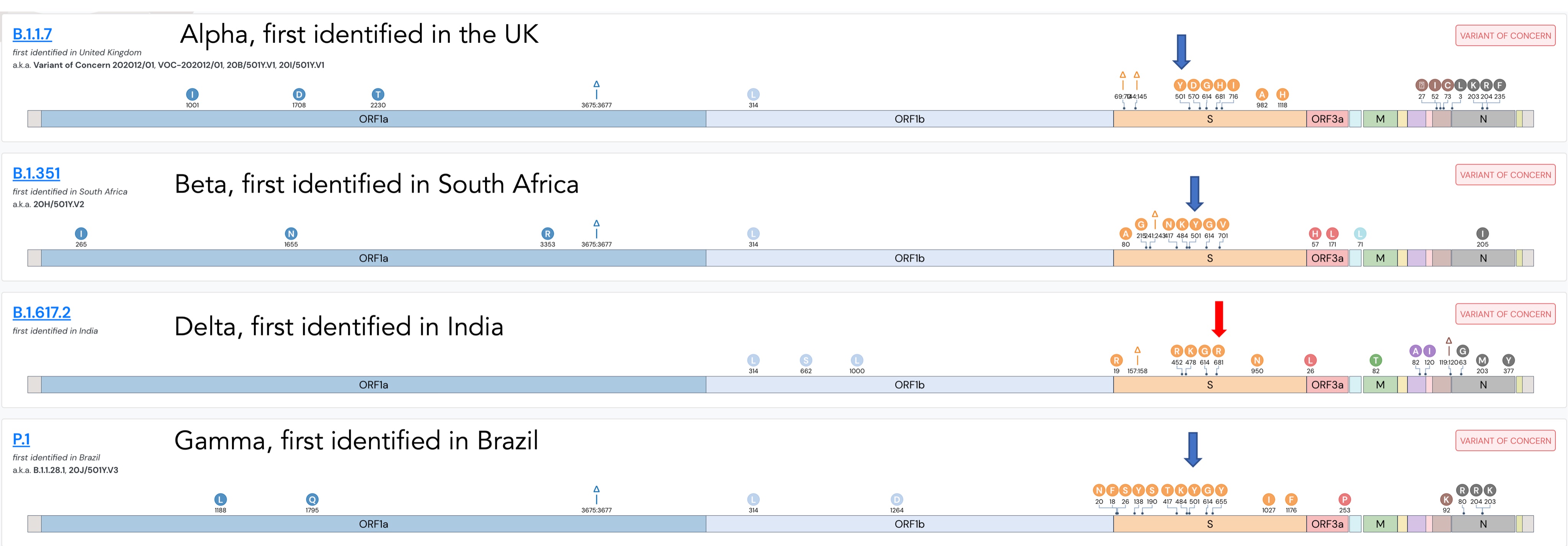
Changes in the virus are monitored by scientists around the world and uploaded to the GISAID database. On the GISAID website, you can see how the SARS-CoV-2 RNA sequence varies progressively, forming branches like a family tree. When a viral strain accumulates significant changes, the WHO classifies it as VARIANT OF INTEREST. When changes in the virus seem to give it the advantage of transmitting better or slipping away from the immune system (antibodies and T cells), the WHO names that virus as a VARIANT OF CONCERN (VOC). For now, there are four variants of concern, including Delta.
The other intervention of the WHO related to the variants has been to name them using the Greek alphabet. Thus, the places where these variants appeared first are not stigmatised. An unfair association that Trump exploited with the «Chinese virus.» Thus, the British, South African, Brazilian, and Indian Variants of Concern (VOC) were named Alpha, Beta, Gamma, and Delta. Something similar would have been necessary if Argentine goalkeeper Fabián Assmann had played in the MSL or the Premier League. Fortunately, Assmann escaped from jokes about his surname by avoiding english-speaking countries. He played in Argentina (Independiente) and Spain (Las Palmas).


Mutations in the spike protein
Among the mutations that modify proteins to improve the virus, the easiest for scientists to explain are those that change, even slightly, the virus’s protein S, also known as the spike protein. Protein S, or spike protein, is what the virus uses to bind to human cells, specifically to ACE2 receptors on the surface of cells. A slight change in the shape or composition of this spike protein can make it easier for the virus to adhere better to human cells and, therefore, to spread more quickly. So it is not surprising that most of the mutations of the variants are located at the spike protein, the key to entry into our cells.

The Delta variant presents S protein mutations already existing in other variants that may improve its infectivity (such as the D614G mutation, which changes *amino acid D to G at position 614), and has novel mutations as the P681R mutation. This mutation changes the amino acid P (Proline) to R (Arginine), which has a positive charge. A study suggests that this P681R mutation may be responsible for the Delta variant replicating faster as it is a critical region for infection. Another recent preprint about P681R suggest the same.
*Amino acids are the «building blocks» with which proteins are built
The Delta variant has taken advantage of some of the best mutations from previous variants and has added other new mutations improving the SARS-CoV-2 replication and transmission.
Delta has changed the match
The higher replication speed of the Delta variant seems to make the incubation period faster, and we have infections with a higher viral load. Thus, it is a bit more challenging to warn and isolating contacts on time. And infected people would be infectious for a longer time. With Delta accounting for most of the infection, the American CDC (Center for Disease Control) recommends (in a note of July 28) that vaccinated people who were in close contact (less than 2 meters for 15 minutes) with an infected person should be tested 3 or 5 days after exposure, and wear a mask at home and indoors for 14 days, or until they have a negative PCR. In addition, it recommends wearing masks in schools, whether you are vaccinated or not. In another report on the Delta variant, the CDC says, «The war has changed.» To understand this change in our match against SARS-CoV-2, we will use the most coveted trophy on the football planet: The World Cup.



In 1930 the first soccer World Cup was played in Uruguay. It was precisely Uruguay who won it, earning the right to have the trophy for the next four years. In 1946, the trophy was named Jules Rimet in honor of the FIFA president. In addition to its sentimental and artistic value (it featured the figure of Nike, the Greek goddess of victory), the cup had an economic value because it was plated in 18-karat gold. The life of the Jules Rimet trophy would work for a movie. It was hidden from the Nazis in Italy during World War II and was stolen and later found by a dog in England before the 1966 World Cup. Brazil owned the Jules Rimet in 1970 after winning the World Cup for the third time. Since then, the FIFA Cup has replaced Jules Rimet Cup, but it did not have a calm life in retirement in Brazil. It was stolen in Rio de Janeiro in 1983 from a bulletproof display case, but apparently not steel lever-proof. The thieves did not give a damn about the delicate carving of the goddess Nike and melted the trophy into the form of gold ingots.
We could make an analogy between the spike protein of the Delta variant and the new FIFA World Cup. Old versions of the virus spike protein will end up disappearing like the Jules Rimet trophy.

The New World Cup, or FIFA Cup, is slightly larger than the Jules Rimet (36.5cm vs 35cm) and has a very different shape. The World Cup will no longer be earned by winning it three times (something Germany did since 1970). The winner’s name is now engraved on the base, and therefore the cup is a bit different every 4 years. Something like this could happen with the spike protein of the Delta variant in the future. The spike protein has changed and can keep changing, adapting better and better to the ACE2 receptors at the surface of human cells in many tissues and organs affected by infection, such as the lungs. If the virus sticks better to the cell, and the virus is transmitted better. This greater transmission capacity of the Delta variant causes us to be infected in circumstances where we were not infected before.

The better coupling of the spike protein would raise the R coefficient (which indicates the transmission capacity without preventive measures) of the SARS-CoV-2 from three to five or six. In other words, each infected person can directly infect an average of six people instead of three. This implies that after three cycles of contagion with the Delta variant, 216 people would be infected instead of 27.
Luckily, the Delta variant has caught us with many vaccinated people, especially the most vulnerable.

And to complete the picture of Delta’s «strengths», the Delta variant reduces the efficacy of vaccines by a small percentage (about 10%). The vaccines are designed for the original SARS-CoV-2, so there will be a percentage of antibodies that will not recognise the Delta variant, but most will. Furthermore, our immune system consists of the humoral system (based on neutralizing antibodies) and the cellular system (based on T cells that kill infected cells). Some studies show that after complete vaccination, the cellular system continues to be effective due to the Delta variant, and the humoral system too although with less efficient antibodies.

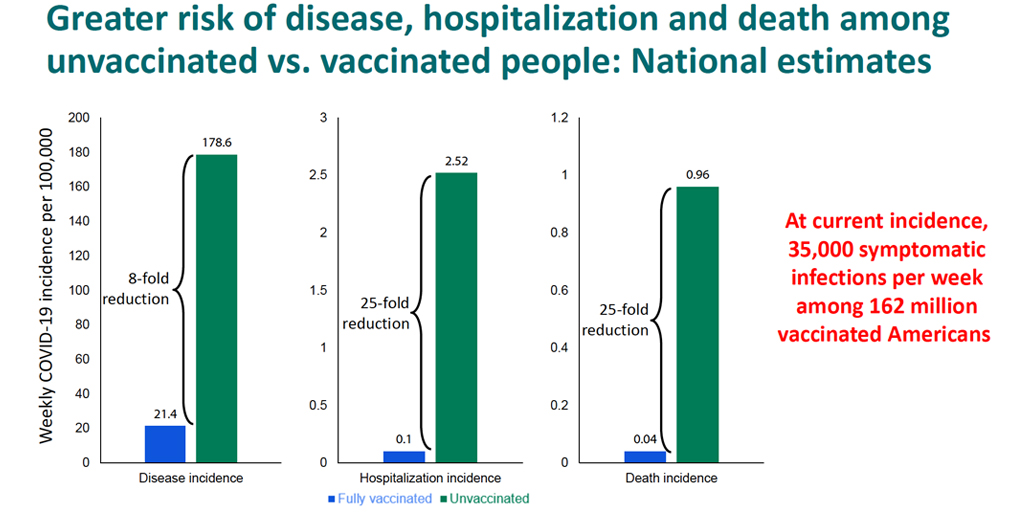
Everything we know about the Delta variant we have learned in a short period of time (Delta appeared a few months ago). Science and epidemiological studies need more time to draw solid conclusions. So far, there is a large handful of data and correlations and a lot of confusion. Delta looks pretty aggressive. Still, in the United Kingdom and Spain, it has been possible to bend the curve of contagion with this variant. In other places (such as in USA states with low percentages of vaccinated), the contagion curve rises exponentially. There are supercontagion events where vaccinated people are infected. However, it seems clear that those vaccinated reduce their viral load earlier, thus reducing their complications and their infective capacity. According to a recent CDC report, the chance of being hospitalised or dying from COVID-19 in double-dose vaccinated is 25 times lower than among unvaccinated. The possibility of being infected is also 8 times less in vaccinated. These vaccines were primarily designed to prevent hospitalisations and deaths. They continue to do that wonderfully against the Delta variant. In any case, we are in a confusing moment of the game. Since the Delta variant seems to make the virus spread better and shows some resistance to vaccines, we need time to relocate to the field and get the ball back.
Vaccines work against the Delta variant as well, and they are still our best weapon. However, we may need to retrieve other tools to finally defeat the virus.
I think Humanity F.C. has a more powerful bench than SARS-CoV-2, and of course, it has more intelligence. We have to play our game with a cool head and avoid a wild confrontation. Such attitude would avoid ending up like that match between Boca Juniors and Sporting de Cristal in 1972, where the referee expelled 19 players. Moreover, all were taken to the police station after the game was suspended.


The Pfizer and AstraZeneca vaccines (two doses) work against the Delta variant. Link to article in the New England Journal of Medicine
A recent study indicates that the effectiveness of Moderna is only reduced by 10% with the Delta variant. Link to the preprint
And yes, the Janssen vaccine, even if it is a single dose, is also effective against the Delta variant. The article has not been published yet, but here you can read the news about the study with almost half a million South African health workers.

What is left on the bench for both teams?
SARS-CoV-2 BENCH
1- NEW VARIANTS
The spike protein can be further modified for a better attachment to the ACE2 receptor. Something like adding ears to the FIFA Cup. In fact, we already heard about the Delta Plus variant with a new mutation in the spike protein (K417N), but there is still no data on its «skills.» It is also possible that changes in the virus will continue to reduce the efficiency of vaccines beyond 10%. Still, they will hardly suddenly cease to be efficient.
Although the probability of new variants appearing is high, the virus’s ability to improve is limited. The WHO has classified more variants of interest (the Greek alphabet will fall short) than variants of concern. Suppose FIFA Cup (36.5 cm) is transformed into the Copa Libertadores (98 cm). In that case, it will be a variant of interest. Still, hardly a variant of concern because a spike protein of that size would not fit into ACE2 receptors.


2- THE ANTI-VACCINES
For example, in Arkansas (USA), 80,000 doses have expired because they cannot find someone to give it to beyond 36% of the vaccinated population.
- THE SELFISHNESS OF THE RICHEST
Now we heard about a third dose. Still, we must not forget that the pandemic is a global problem and that «only» 15% of the world population has two doses of vaccine, and 30% have one dose. That is why voices suggest giving the third dose only to patients at risk, such as the immunosuppressed, and offering as many vaccines as possible to countries with low percentages of vaccinated population. For example, Argentina and India, two countries that never met in an official match, only in the Nheru Cup in 1984, have 15 and 10% of the population vaccinated, respectively.
BENCH OF HUMANITY F.C
1- VACCINES 1.0
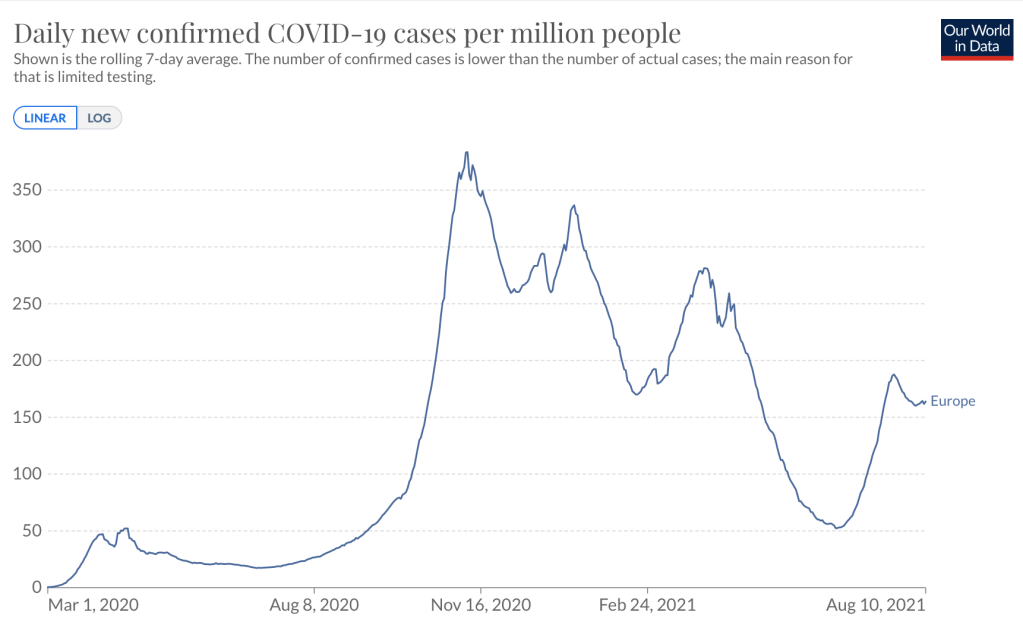
Vaccines work! For example, Europe has seen 5 waves of infections but the last wave is not associated with a wave of fatalities. This happened thanks to vaccines. It happens that they are not as effective in preventing infections as in avoiding hospitalizations and deaths. But our best weapons are still vaccines, and we must take advantage of them. The more vaccinated people, the better for everyone and the worse for the virus because we reduce its ability to mutate. According to recent compiled data, the CDC also recommend the vaccination while pregnant or breastfeeding. Therefore, you must first convince the undecided, respecting their ideas and fears. Then there is the possibility of vaccinating children between the ages of 12 and 18 as RNA vaccines have been tested in clinical trials and approved for use in this age range. Countries such as the United States, Israel, or Spain are already vaccinating children under 18. In other places such as the United Kingdom, they are still thinking about it because they think the benefits are more for the community than for the children. They argue that in the UK «only» 30 children under 18 died from COVID-19 from February 2020 to March 2021. Still, 30 children seem like a lot to me. In addition, there are studies underway to assess the impact of «Long COVID-19» in children, which is estimated to affect 10-15% of infected children.
With the arrival of the school year, vaccinating minors (12 to 18 years old) would protect them from the rare but possible complications of COVID-19 and would help the rest of the population to stop transmission. On the other hand, the advantage of vaccinating minors for the rest of the population is clear. By increasing the Ro or transmissibility of the virus, the proportion of the people necessary to achieve herd immunity increases, in which the vaccinated act as a firewall until the virus is extinguished. Perhaps 80-90% vaccinated are now needed instead of 70-80%. Or maybe it will be hard to reach herd immunity with our present weapons, but it is worth trying. For those under 12, clinical trials are being carried out, but it may not be necessary because we know that they are contagious and transmit little.

2- VACCINES 2.0
RNA and DNA vaccines can be easily adapted to new variants. In fact, Pfizer is already developing a variant of the vaccine against the Delta variant. On the other hand, sterilizing vaccines are yet to arrive. In addition to protecting us from complications from COVID-19, sterilizing vaccines would also slow down the ability to spread. These vaccines are intranasal and activate B and T lymphocytes of the respiratory mucosa, which is why they act earlier, preventing the infected person from spreading the virus. Of about hundred COVID-19 vaccines that are in clinical trials, only seven are sterilizing.
3- TEST
The tests are still an excellent ally to fight the virus. The test allows us to detect and isolate the infected person before they infect. They are becoming more accessible and affordable. The higher viral load of the Delta variant may mean that rapid antigen tests would give fewer false negatives. The value of tests to stop transmission is well known in China. Recently, after an outbreak that infected 200 people at the Nanjing airport, a city of about 9 million inhabitants, they have carried out three rounds of tests on the entire population to stop the outbreak at its roots.
4- MASKS AND COMMON SENSE
Vaccine immunity seems to be lasting, but we are becoming a heterogeneous population in terms of our immune systems against SARS-CoV-2. We have received different vaccines and at distinct times. We have also been exposed to the virus in different ways. This means that an outbreak in a group of vaccinated people would infect some people but not others. These events create confusion in a heterogeneous population. With the Delta variant, it is increasingly difficult to predict the risk of events. Carrying a mask on hand and wearing it indoors sounds reasonable as long as there are infections in your area. Another common sense act is knowing how to say NO to a social gathering if you have symptoms and get tested as soon as possible. The fact that the Delta variant replicates so quickly can help reduce the asymptomatic and contagious time.
CONCLUSION
There are indeed cases of vaccinated people who become infected with an initial viral load similar to those not vaccinated. However, vaccinated people drop that burden quickly, and there is much evidence that they are protected from severe disease. Therefore, vaccines, even with the Delta variant, reduce the transmission of the virus, reduce hospitalizations and, most importantly, protect against death from COVID-19. Thus, being vaccines our best weapon, we have to vaccinate as many people as possible.
When the opposing team begins to shake off the pressure, we need to push a little more to gain confidence. SARS-CoV-2 has made an excellent strategic move with the Delta variant. Delta is fast, but Usain Bolt was also fast too, but a bad player at Australian A-League soccer with the Central Coast Mariners. Humanity F. C. is far superior to SARS-CoV-2, but we have to recover the ball to set the game’s pace. Don’t be passive. Help your team. Be supportive. Show up asking the ball to your teammates, and touch, touch, and touch to dominate and win this match.
@CeronLab
@raticosdefutbol
ANNEX:
Evergrande Academy
USAIN BOLT PLAYING FOOTBALL
India vs Argentina 1984
